
di Davide Pacini
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spread rapidly from China to the other Countries worldwide and on the March 11th 2020 the WHO declared the so-called COVID-19 a pandemic. In Italy, first cases of COVID-19 occurred at the end of January and on 24th of May there were a total of 229,858 infected patients with 32,785 deaths (about 14,2% of the total)representing the third Country for the number of infections, after USA and Spain.
Due to the high contagiousness of SARS-CoV-2 virus, a significant increase of hospitalizations occurred. Moreover, hospital systems had to reduce general health services prioritizing the  treatment for severe and high-risk non-COVID-19 patients modifying the wards’ organizations with an important resource consumption. Surgery units stopped to treat elective cases in order to focus on urgent and emergent patients to minimize Intensive Care Unit (ICU) beds utilization. Thus, the waiting list keeps on growing and the conditions of patients awaiting for the delayed operation are getting worse, resulting in an increase of the surgical risk. Moreover, repurposing cardiac ICUs as medical ICUs for treating COVID-19 patients could limit the specialty care for cardiovascular patients.
treatment for severe and high-risk non-COVID-19 patients modifying the wards’ organizations with an important resource consumption. Surgery units stopped to treat elective cases in order to focus on urgent and emergent patients to minimize Intensive Care Unit (ICU) beds utilization. Thus, the waiting list keeps on growing and the conditions of patients awaiting for the delayed operation are getting worse, resulting in an increase of the surgical risk. Moreover, repurposing cardiac ICUs as medical ICUs for treating COVID-19 patients could limit the specialty care for cardiovascular patients.
Patients with underlying cardiovascular diseases have an increased risk of developing into the severe form of COVID-19 and, on the other hand, COVID-19 is associated with increased incidence of acute cardiac injury. The higher mortality rate is found in males, age > 60 years with underlying common comorbities such as diabetes mellitus and cardiac or lung disorders. Thus, adult cardiac surgery patients are considered a very high-risk population because they usually fall in that category. A nosocomial SARS-CoV-2 infection could be easily lethal in this delicate population. Moreover, health care workers are exposed to the risk of contagion or they could become vectors of virus transmission.
In our Country the infection didn’t spread evenly, focusing specially in the North of the Country. Italian government took containment measures for Regions with outbreak of infection and, on March 9th, a complete nationwide lock-down was imposed. Lombardy is the Region with the major number of positive patients. Out of the 20 Cardiac Surgery centers in Lombardy, 16 centers closed and now work as spoke units for the remaining 4 that are considered the “hubs”. Emergent/urgent patients are sent from the spoke units to the hubs to be treated.
Emilia Romagna is the third Region in Italy for the number of infections, after Lombardy and Piedmont, and the S. Orsola Hospital, University of Bologna, became one of the main 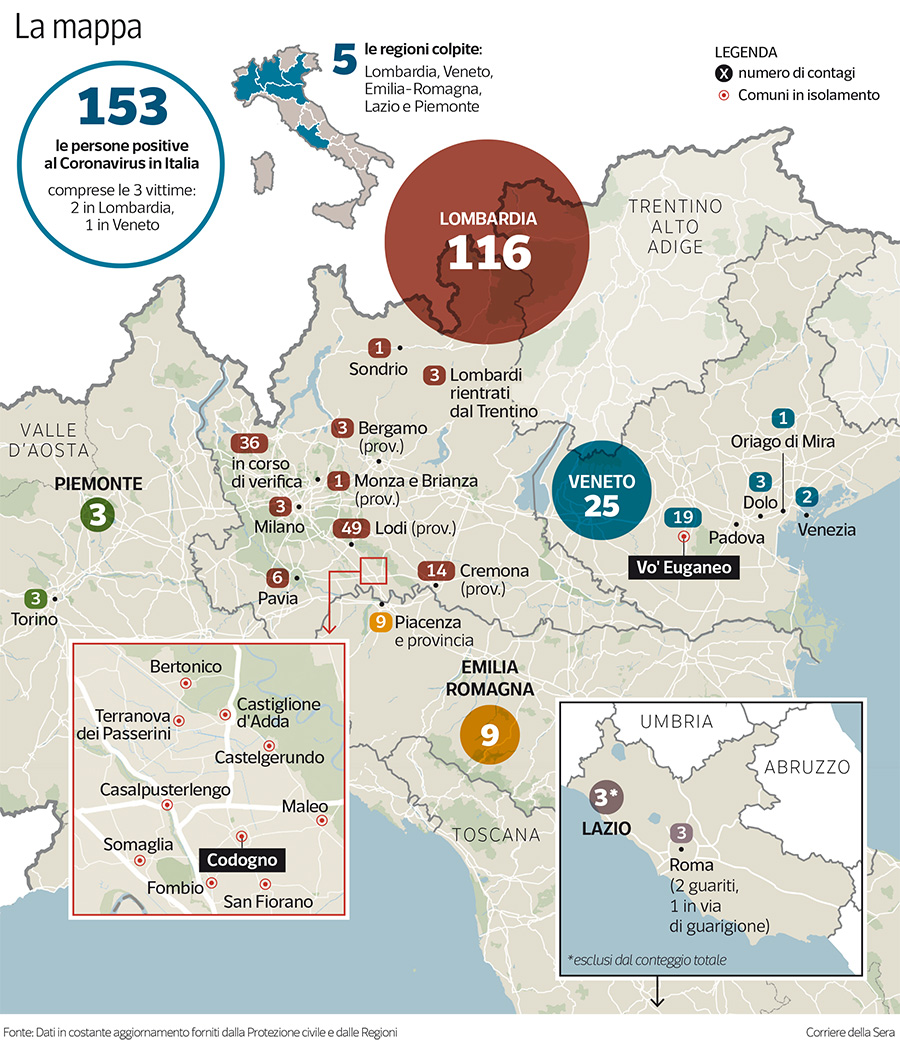 regional Hub centers attending COVID-19 network. In our department, we established an important cooperation with the Hospital Administration in order to keep the cardiac surgery activity open even during the peak of pandemic. Our ICU was 75% dedicated to COVID-19 patients as well as our ward was reorganized with a preference towards infected non-cardiac-surgery patients. Between January 1st and April 30th a total of 273 adult patients underwent cardiac surgery procedures in our center. During January and February we were able to perform 4-5 operations per day (a total of 79 and 85 procedures, respectively) while in March and April we had to reduce to 1 procedure per day. In order to face the drastic reduction in the surgical activity we established a cooperation with a “COVID-free” private clinic near our hospital where we could perform 1-2 daily operations more. In that way we were able to contain the reduction of the surgical activity by only 30%. A total of 59 and 51 patients were treated during March and April, respectively.
regional Hub centers attending COVID-19 network. In our department, we established an important cooperation with the Hospital Administration in order to keep the cardiac surgery activity open even during the peak of pandemic. Our ICU was 75% dedicated to COVID-19 patients as well as our ward was reorganized with a preference towards infected non-cardiac-surgery patients. Between January 1st and April 30th a total of 273 adult patients underwent cardiac surgery procedures in our center. During January and February we were able to perform 4-5 operations per day (a total of 79 and 85 procedures, respectively) while in March and April we had to reduce to 1 procedure per day. In order to face the drastic reduction in the surgical activity we established a cooperation with a “COVID-free” private clinic near our hospital where we could perform 1-2 daily operations more. In that way we were able to contain the reduction of the surgical activity by only 30%. A total of 59 and 51 patients were treated during March and April, respectively.
The patients who were treated were only urgent/emergent cases and those with cardiac disease whose treatment was considered not to be postponed more than a month. In the private clinic we were able to treat also some elective patients who were in waiting list since more than a year. Acute aortic syndromes were 19 (6,9%). The heart failure surgical program didn’t stop and we performed 8 heart transplant, 3 LVAD implant and 3 pulmonary artery thromboembolectomy.
In-hospital mortality was 1,1% (N=3/273). None of our patients were infected by SARS-CoV-2 during hospitalization. Four patients (1,4%) became positive during the postoperative rehabilitation in other hospitals and one of those died (N = 1/4).
Actually, in our center, each patient undergoes nasal swab one day before the hospitalization. If the swab is positive the patient is not admitted and the operation is postponed. If there’s an emergent case, a nasal swab is performed at the time of admission and the patient is considered COVID-19 suspect until the result of the swab is available. If we have to perform a cardiac transplant, the recipient is admitted and he undergoes nasal swab test and HRCT of the chest before considering him suitable for the operation. We created a specific “COVID-19 route” for suspected patients with dedicated ICU beds and one operation room to perform cardiac operations. Surgeons must wear visors and specific protective masks during the procedure, while all the materials needed are kept in the operation room or passed by outside-nurses trying to limit the door opening as much as possible.
At the time of writing, here in Italy, new COVID-19 cases have begun to decline showing a “flattening of the curve”. Deciding when and how to resume non-urgent health care delivery can be challenging. However, we strongly think that hospital systems should put effort in reorganizing the resources. COVID-19 slowed down our Country but cardiac surgery has to find a way to ramp up again for the sake of patients awaiting for their treatment.
